Dyadic Developmental Psychotherapy, an attachment-based therapy is an evidence-based treatment for children with Trauma-Attachment Disorders, Reactive Attachment Disorder, and other disorders of attachment that are complicated by severe trauma or histories of maltreatment. See the Center for Family Development's study in the March 2006 issue of Child and Adolescent Social Work, a professional peer-reviewed journal.
The Center for Family Development has completed a research study following children after treatment and have found that Dyadic Developmental Psychotherapy is an effective treatment method for children with trauma-attachment disorders.
Treatment for Children with Reactive Attachment Disorder: Dyadic Developmental Psychotherapy
Dyadic Developmental Psychotherapy (DDP) is an approach to treating disorders of attachment based on attachment theory and research. Previously it was found that, one year after treatment ended, children who received DDP had clinically and statistically significant improvements while those in the control group did not. This study extends those results out to 4 years. The treatment group’s scores on the Child Behavior Checklist (CBCL) remained in the normal range. The control group’s scores on several scales worsened to a statistically significant degree, despite the fact that they received treatment from other providers during the intervening period, averaging 50 sessions.
Introduction
Children with histories of maltreatment, such as physical and psychological neglect, physical abuse, and sexual abuse, are at risk of developing severe psychiatric problems (Gauthier et al., 1996; Malinosky-Rummell and Hansen, 1993). In particular, they are likely to develop Reactive Attachment Disorder (RAD) (Lyons- Ruth and Jacobvitz, 1999; Greenberg, 1999). The trauma experienced is the result of abuse or neglect, inflicted by a primary caregiver, which disrupts the normal development of secure attachment. Such children are at risk of developing disorganized attachment (Carlson, et al., 1995; Lyons-Ruth and Jacobvitz 1999; Solomon and George, 1999; Main and Hesse, 1990), which is associated with a number of developmental problems, including dissociative symptoms (Carlson, 1988), as well as depressive, anxiety, and acting-out symptoms (Lyons-Ruth, 1996; Lyons- Ruth, Alpern, and Repacholi, 1993). The term ‘disorganized attachment’ is a research category used to describe a pattern and style of attachment behavior and the attachment system. The term ‘Reactive Attachment Disorder’ is a psychiatric diagnosis defined by criteria in the DSM-IV (APA, 1994).
Many children with histories of maltreatment are violent (Robins, 1978) and aggressive (Prino and Peyrot, 1994) and as adults are at risk of developing a variety of psychological problems (Schreiber and Lyddon, 1998) and personality disorders, including antisocial personality disorder (Finzi et al., 2000), narcissistic personality disorder, borderline personality disorder, and psychopathic personality disorder (Dozier, Stovall, and Albus, 1999). Neglected children are at risk of social withdrawal, social rejection, and pervasive feelings of incompetence (Finzi et al., 2000). Children who have histories of abuse and neglect are at significant risk of developing Post Traumatic Stress Disorder as adults (Allan, 2001; Andrews et al., 2000). Children who have been sexually abused are at significant risk of developing anxiety disorders (2.0 times the average), major depressive disorders (3.4 times average), alcohol abuse. (2.5 times average), drug abuse (3.8 times average), and antisocial behavior (4.3 times average) (MacMillian, 2001). The effective treatment of such children is a public health concern (Walker, Goodwin, and Warren, 1992).
The best predictor of a child’s attachment classification is the state of mind with respect to attachment of the birth mother (Lyons- Ruth and Jacobvitz, 1999). A birth mother’s attachment classification before the birth of her child can predict with 80% accuracy her child’s attachment classification at 6 years of age (Main and Cassidy, 1988). Finally, recent research by Dozier (2001) found that the attachment classification of a foster mother has a profound effect on the attachment classification of the child. She found that the child’s attachment classification becomes similar to that of the foster mother after 8 months in placement. These findings strongly argue for a non-genetic mechanism for the transmission of attachment patterns across generations and for the beneficial impact of a healing and healthy relationship.
These findings also strongly suggest that effective treatment requires an affectively attuned relationship (Becker-Weidman, 2005). Siegel (1999, p. 333) stated, ‘As parents reflect with their securely attached children on the mental states that create their shared subjective experience, they are joining with them in an important co-constructive process of understanding how the mind functions. The inherent feature of secure attachment – contingent, collaborative communication – is also a fundamental component in how interpersonal relationships facilitate internal integration in a child. This has implications for the effective treatment of maltreated children. For example, when in a therapeutic relationship the child is able to reflect upon aspects of traumatic memories and experiences without becoming dysregulated, the child develops an expanded capacity to tolerate increasing amounts of affect. The therapist or parent dyadically regulates the child’s level of arousal and affect, keeping the child regulated. Over time, the child internalizes this and so becomes able to self-regulate. This process is similar to what is seen in the healthy infant-parent relationship, where the parent regulates the infant’s states of arousal to maintain homeostasis. The attuned resonant relationship between child and therapist and child and caregiver enables the child to make sense out of memories, autobiographical representations, and affect.
Dyadic Developmental Psychotherapy (DDP) shares many important elements with optimal, sound clinical practice. For example, attention to the dignity of the client, respect for the client’s experiences, and starting where the client is are all time honored principles of social work practice and all are also central elements of DDP. What distinguishes DDP from other clinical work with children is the strong emphasis on maintaining a positive affectively attuned relationship with the child, a deep acceptance of the child’s affect and experience, and greater emphasis on experience and process rather than on verbalization and content. The practice of DDP requires the clinician to become affectively attuned with the child and caregivers, and to develop and maintain a meaningful emotional connection with the child, often at a non-verbal and experiential level. DDP requires a greater use of self than, for example, cognitive-behavioral psychotherapy, behavioral approaches, or strategic or structural family therapy interventions. However, it shares many basic principles of treatment with these other approaches.
In a previous study (Becker-Weidman, 2006), it was found that DDP was an effective treatment for children with Reactive Attachment Disorder (RAD). Children were assessed at two time points. Selection criteria were all cases during a 12-month period of time in which the child met the DSM IV criteria for a primary diagnosis of RAD. Children in the treatment group received DDP at the Center for Family Development. Children in the control group were only evaluated and did not receive DDP, although 53% of these children received treatment from other providers not affiliated with the Center (usual care). Children in both groups had significant histories of physical abuse, physical or psychological neglect, sexual abuse, or institutional care and were experiencing Complex Post Traumatic Stress Disorder. All children were between the ages of 5 years old and 16 years at the time treatment began. Most had at least one prior episode of treatment, with the average being 3.4 prior treatment episodes for the treatment group and 2.7 prior treatment episodes for the control group. All children resided with caregivers. In the treatment group, 26 lived with adoptive parents and 8 with foster parents. In the control group, 24 resided with adoptive parents and 6 with foster parents. In the treatment group, 24 are male and 10 are female; in the control group, 14 are male and 16 are female.
Post-test measures were administered a little over one year after treatment ended for the treatment group. Thirty-five follow-up questionnaires were mailed to the treatment group and 34 were returned. Thirty out of 34 questionnaires mailed to the control group were returned. One family in the treatment group had moved and there was no forwarding address. Two families in the control group had moved without leaving a forwarding address and two families declined to participate. All participants completed the questionnaires during an evaluation process involving three sessions: two with the primary caregivers and one with the child, the administration of various psychological tests, and a thorough review of all records and previous evaluations.
The children in foster care had all been residing with their foster parents for more than one year. On the demographic variables measured (age at placement, gender, race, number of prior treatment episodes, age when treatment or the evaluation occurred, and length of follow-up time period), the foster children and adopted children were not statistically different. There were no statistically significant differences between the treatment and control groups on either the demographic variables measures or on the pre-treatment scores on the Child Behavior Checklist and the Randolph Attachment Disorder Questionnaire. There were clinically and statistically significant reductions in behaviors as measured by the Child Behavior Checklist (CBCL, Achenbach, 1991) and the Randolph Attachment Disorder Questionnaire (Randolph, 2000) among those receiving DDP. Children in the control group, about 50% of whom received ‘usual care’ such as play therapy, family therapy, individual therapy, and residential treatment in the time between the initial data collection and the follow-up data collection, showed no clinically or statistically significant changes in the measured behaviors. The children in the control group who received ‘usual care’ received treatment from other agencies or private practitioners not associated with the Center for Family Development.
The current study explored the question of whether the positive changes in behavior seen in the treatment group after one year continued. The longer-term effects of DDP were explored by comparing the initial scores on the CBCL and Randolph Attachment Disorder Questionnaire for the treatment and control groups with the scores for these groups after 3–4 years.
Method
Questionnaires were mailed to the children for whom there was follow-up information in the original study. The average follow-up period was approximately 4 years for those in the treatment group. About two-thirds of the families could be located and returned the questionnaires (24 of 34 for the treatment group and 20 out of 30 for the control group). Most of the families from whom we did not receive questionnaires had moved and we were unable to locate their new address. This study is preliminary and exploratory.
One hundred percent of the control group families had sought and continued in treatment with other treatment providers, with an average of 50 sessions. None of these families received DDP. As will be shown, despite receiving extensive treatment, the control group actually exhibited an increase in symptoms over the 3.3 years. Forty-two percent of the treatment group received treatment after completing DDP. Most of this continued treatment was for co-morbid conditions, such as Bipolar Disorder and Attention Deficit/Hyperactivity Disorder. The majority of the children in the treatment group who received continued treatment after competing DDP received medication management treatment.
Participants
Details about sample selection can be found in Becker-Weidman (2006). The average age at adoption was 7 years and the average number of episodes of prior treatment was 3.4 (82% of the children in the treatment group and 83% of children in the control group had previously received treatment, but without improvement in symptoms). Families were referred to the Center for Family Development from a variety of sources including departments of social services, physician offices, other mental health providers and clinics, and ‘word of mouth’. All cases selected were from the closed cases files during a one-year period and all children had a primary diagnosis of RAD using the criteria in the DSM IV.
Measures
The Child Behavior Checklist (CBCL) (Achenbach, 1991) is composed of several questionnaires and is a parent-report measure designed to assess behavior problems of children 2 to 18 years of age. The instrument has widely accepted reliability and validity that is reported on extensively in the manual.
The Randolph Attachment Disorder Questionnaire (Randolph, 2000) assesses Attachment Disorder. It consists of 30 items completed by the caregiver who rates each item on a 1–5 scale. The manual (Randolph, 2000) describes in detail the development of the test, scoring, reliability, and validity.
Independent Variable: Dyadic Developmental Psychotherapy
Dyadic Developmental Psychotherapy (Hughes, 1997, 2004, 2005) basic principles are summarized as follows:
1. A focus on both the caregivers’ and therapists’ own attachment strategies. Previous research (Dozier et al., 2001; Tyrell et al., 1999) has shown the importance of the caregiver’s and therapist’s state of mind for the success of interventions.
2. Therapist and caregiver are attuned to the child’s subjective experience and reflect this back to the child. In the process of maintaining an intersubjective attuned connection with the child, the therapist and caregiver help the child regulate affect and construct a coherent autobiographical narrative.
3. Sharing of subjective experiences.
4. Use of PACE and PLACE are essential to healing. PACE refers to the therapist setting a healing pace to therapy by being playful, accepting, curious, and empathic. The idea is that the therapist maintains an emotional connection with the client (attunement) and dyadically regulates the child’s affect. In this manner, the therapist ensures that there is an emotionally meaningful component to treatment without the client becoming dysregulated. PLACE refers to the parent creating a healing environment by being playful, loving, accepting, curious, and empathic. These ideas are described more fully below.
1. Directly address the inevitable misattunements and conflicts that arise in interpersonal relationships.
2. Caregivers use attachment-facilitating interventions.
3. Use of a variety of interventions, including cognitive-behavioral strategies.
Dyadic Developmental Psychotherapy interventions flow from several theoretical and empirical lines (Becker-Weidman and Shell, 2005). Attachment theory (Bowlby, 1980, 1988) provides the theoretical foundation for DDP. Early trauma disrupts the normally developing attachment system by creating distorted internal working models of self, others, and caregivers.
Current thinking and research on the neurobiology of interpersonal behavior (Siegel, 1999, 2001, 2002; Schore, 2001) is another part of the foundation on which DDP rests. The work of Bruce Perry (Perry, 1994) and the Child Trauma Academy describes how trauma affects the developing child in a profound manner and requires special treatment approaches. The works of Siegel, Shore, and others provide a foundation for understanding how early attachment experiences affect brain development and later behavior. The focus of this work on the nature and quality of the attachment relationship support a major focus of DDP of maintaining a positive affectively attuned relationship as central to healing trauma.
The primary approach is to create a secure base in treatment (using techniques that fit with maintaining a healing PACE (Playful, Accepting, Curious, and Empathic) and at home using principles that provide safe structure and a healing PLACE (Playful, Loving, Acceptance, Curious, and Empathic). Developing and sustaining an attuned relationship within which contingent collaborative communication occurs helps the child heal. Healing is facilitated by the co-regulation of affect and the development of greater reflective capacities (Fonagy et al., 2002).
Dyadic Developmental Psychotherapy, as conducted at the Center for Family Development, uses 2-hour sessions involving one therapist, parent(s), and child. Two offices are used. Unless the caregivers are in the treatment room, the caregivers view treatment from another room by closed circuit television or a one-way mirror. The usual structure of a session involves three components. First, the therapist meets with the caregiver in one office while the child is seated in the treatment room. During this part of treatment, the caregiver is instructed in attachment parenting methods (Becker-Weidman and Shell, 2005). The caregiver’s own issues that may create difficulties with developing affective attunement with their child may also be explored and resolved. Effective parenting methods for children with trauma-attachment disorders require a high degree of structure and consistency, along with an affective milieu that demonstrates playfulness, love, acceptance, curiosity, and empathy (PLACE). During this part of the treatment, caregivers receive support and are given the same level of attuned responsiveness that we wish the child to experience. Quite often caregivers feel blamed, devalued, incompetent, depleted, and angry. Parent-support is an important dimension of treatment to help caregivers be more able to maintain an attuned connecting relationship with their child. Second, the therapist, frequently with the caregiver present as well, meets with the child in the treatment room. This generally takes 60–90 minutes. Third, the therapist meets with the caregiver without the child. Broadly speaking, the treatment with the child uses three categories of interventions: affective attunement, cognitive restructuring, and psychodramatic reenactments. Treatment with the caregivers uses two categories of interventions: first, teaching effective parenting methods and helping the caregivers avoid power struggles and, second, maintaining the proper PLACE or attitude. The caregivers provide a high degree of structure to provide safety for the child. Within this structured world, the caregiver maintains a high degree of affective attunement that is nurturing and that repeatedly enacts the attachment-cycle of engagement, disruption, and interactive repair (Siegel, 2001; Schore, 2001).
The treatment provided in this study (DDP) often adhered to a structure with several dimensions (see Figure 1). First, behavior is identified and explored. The behavior may have occurred in the immediate interaction or have occurred at some time in the past. Second, using curiosity and acceptance the behavior is explored and the meaning to the child begins to emerge. Third, empathy is used to reduce the child’s sense of shame and increase the child’s sense of being accepted and understood. Fourth, the child’s behavior is then normalized. In other words, once the meaning of the behavior and its basis in past trauma is identified, it becomes understandable that the symptom is present. An example of such an interaction is the following:
Therapist: ‘Wow, I see how you got so angry when your Mom asked you to pick up your toys. You thought she was being mean and didn’t want you to have fun or love you. You thought she was going to take everything away and leave you like your first Mom did, like when your first Mom took your toys and then left you alone in the apartment that time. Oh, I can really understand now how hard that must be for you when Mom said to clean up. You really felt mad and scared. That must be so hard for you.’
The Center for Family Development has completed a research study following children after treatment and have found that Dyadic Developmental Psychotherapy is an effective treatment method for children with trauma-attachment disorders.
Treatment for Children with Reactive Attachment Disorder: Dyadic Developmental Psychotherapy
Dyadic Developmental Psychotherapy (DDP) is an approach to treating disorders of attachment based on attachment theory and research. Previously it was found that, one year after treatment ended, children who received DDP had clinically and statistically significant improvements while those in the control group did not. This study extends those results out to 4 years. The treatment group’s scores on the Child Behavior Checklist (CBCL) remained in the normal range. The control group’s scores on several scales worsened to a statistically significant degree, despite the fact that they received treatment from other providers during the intervening period, averaging 50 sessions.
Introduction
Children with histories of maltreatment, such as physical and psychological neglect, physical abuse, and sexual abuse, are at risk of developing severe psychiatric problems (Gauthier et al., 1996; Malinosky-Rummell and Hansen, 1993). In particular, they are likely to develop Reactive Attachment Disorder (RAD) (Lyons- Ruth and Jacobvitz, 1999; Greenberg, 1999). The trauma experienced is the result of abuse or neglect, inflicted by a primary caregiver, which disrupts the normal development of secure attachment. Such children are at risk of developing disorganized attachment (Carlson, et al., 1995; Lyons-Ruth and Jacobvitz 1999; Solomon and George, 1999; Main and Hesse, 1990), which is associated with a number of developmental problems, including dissociative symptoms (Carlson, 1988), as well as depressive, anxiety, and acting-out symptoms (Lyons-Ruth, 1996; Lyons- Ruth, Alpern, and Repacholi, 1993). The term ‘disorganized attachment’ is a research category used to describe a pattern and style of attachment behavior and the attachment system. The term ‘Reactive Attachment Disorder’ is a psychiatric diagnosis defined by criteria in the DSM-IV (APA, 1994).
Many children with histories of maltreatment are violent (Robins, 1978) and aggressive (Prino and Peyrot, 1994) and as adults are at risk of developing a variety of psychological problems (Schreiber and Lyddon, 1998) and personality disorders, including antisocial personality disorder (Finzi et al., 2000), narcissistic personality disorder, borderline personality disorder, and psychopathic personality disorder (Dozier, Stovall, and Albus, 1999). Neglected children are at risk of social withdrawal, social rejection, and pervasive feelings of incompetence (Finzi et al., 2000). Children who have histories of abuse and neglect are at significant risk of developing Post Traumatic Stress Disorder as adults (Allan, 2001; Andrews et al., 2000). Children who have been sexually abused are at significant risk of developing anxiety disorders (2.0 times the average), major depressive disorders (3.4 times average), alcohol abuse. (2.5 times average), drug abuse (3.8 times average), and antisocial behavior (4.3 times average) (MacMillian, 2001). The effective treatment of such children is a public health concern (Walker, Goodwin, and Warren, 1992).
The best predictor of a child’s attachment classification is the state of mind with respect to attachment of the birth mother (Lyons- Ruth and Jacobvitz, 1999). A birth mother’s attachment classification before the birth of her child can predict with 80% accuracy her child’s attachment classification at 6 years of age (Main and Cassidy, 1988). Finally, recent research by Dozier (2001) found that the attachment classification of a foster mother has a profound effect on the attachment classification of the child. She found that the child’s attachment classification becomes similar to that of the foster mother after 8 months in placement. These findings strongly argue for a non-genetic mechanism for the transmission of attachment patterns across generations and for the beneficial impact of a healing and healthy relationship.
These findings also strongly suggest that effective treatment requires an affectively attuned relationship (Becker-Weidman, 2005). Siegel (1999, p. 333) stated, ‘As parents reflect with their securely attached children on the mental states that create their shared subjective experience, they are joining with them in an important co-constructive process of understanding how the mind functions. The inherent feature of secure attachment – contingent, collaborative communication – is also a fundamental component in how interpersonal relationships facilitate internal integration in a child. This has implications for the effective treatment of maltreated children. For example, when in a therapeutic relationship the child is able to reflect upon aspects of traumatic memories and experiences without becoming dysregulated, the child develops an expanded capacity to tolerate increasing amounts of affect. The therapist or parent dyadically regulates the child’s level of arousal and affect, keeping the child regulated. Over time, the child internalizes this and so becomes able to self-regulate. This process is similar to what is seen in the healthy infant-parent relationship, where the parent regulates the infant’s states of arousal to maintain homeostasis. The attuned resonant relationship between child and therapist and child and caregiver enables the child to make sense out of memories, autobiographical representations, and affect.
Dyadic Developmental Psychotherapy (DDP) shares many important elements with optimal, sound clinical practice. For example, attention to the dignity of the client, respect for the client’s experiences, and starting where the client is are all time honored principles of social work practice and all are also central elements of DDP. What distinguishes DDP from other clinical work with children is the strong emphasis on maintaining a positive affectively attuned relationship with the child, a deep acceptance of the child’s affect and experience, and greater emphasis on experience and process rather than on verbalization and content. The practice of DDP requires the clinician to become affectively attuned with the child and caregivers, and to develop and maintain a meaningful emotional connection with the child, often at a non-verbal and experiential level. DDP requires a greater use of self than, for example, cognitive-behavioral psychotherapy, behavioral approaches, or strategic or structural family therapy interventions. However, it shares many basic principles of treatment with these other approaches.
In a previous study (Becker-Weidman, 2006), it was found that DDP was an effective treatment for children with Reactive Attachment Disorder (RAD). Children were assessed at two time points. Selection criteria were all cases during a 12-month period of time in which the child met the DSM IV criteria for a primary diagnosis of RAD. Children in the treatment group received DDP at the Center for Family Development. Children in the control group were only evaluated and did not receive DDP, although 53% of these children received treatment from other providers not affiliated with the Center (usual care). Children in both groups had significant histories of physical abuse, physical or psychological neglect, sexual abuse, or institutional care and were experiencing Complex Post Traumatic Stress Disorder. All children were between the ages of 5 years old and 16 years at the time treatment began. Most had at least one prior episode of treatment, with the average being 3.4 prior treatment episodes for the treatment group and 2.7 prior treatment episodes for the control group. All children resided with caregivers. In the treatment group, 26 lived with adoptive parents and 8 with foster parents. In the control group, 24 resided with adoptive parents and 6 with foster parents. In the treatment group, 24 are male and 10 are female; in the control group, 14 are male and 16 are female.
Post-test measures were administered a little over one year after treatment ended for the treatment group. Thirty-five follow-up questionnaires were mailed to the treatment group and 34 were returned. Thirty out of 34 questionnaires mailed to the control group were returned. One family in the treatment group had moved and there was no forwarding address. Two families in the control group had moved without leaving a forwarding address and two families declined to participate. All participants completed the questionnaires during an evaluation process involving three sessions: two with the primary caregivers and one with the child, the administration of various psychological tests, and a thorough review of all records and previous evaluations.
The children in foster care had all been residing with their foster parents for more than one year. On the demographic variables measured (age at placement, gender, race, number of prior treatment episodes, age when treatment or the evaluation occurred, and length of follow-up time period), the foster children and adopted children were not statistically different. There were no statistically significant differences between the treatment and control groups on either the demographic variables measures or on the pre-treatment scores on the Child Behavior Checklist and the Randolph Attachment Disorder Questionnaire. There were clinically and statistically significant reductions in behaviors as measured by the Child Behavior Checklist (CBCL, Achenbach, 1991) and the Randolph Attachment Disorder Questionnaire (Randolph, 2000) among those receiving DDP. Children in the control group, about 50% of whom received ‘usual care’ such as play therapy, family therapy, individual therapy, and residential treatment in the time between the initial data collection and the follow-up data collection, showed no clinically or statistically significant changes in the measured behaviors. The children in the control group who received ‘usual care’ received treatment from other agencies or private practitioners not associated with the Center for Family Development.
The current study explored the question of whether the positive changes in behavior seen in the treatment group after one year continued. The longer-term effects of DDP were explored by comparing the initial scores on the CBCL and Randolph Attachment Disorder Questionnaire for the treatment and control groups with the scores for these groups after 3–4 years.
Method
Questionnaires were mailed to the children for whom there was follow-up information in the original study. The average follow-up period was approximately 4 years for those in the treatment group. About two-thirds of the families could be located and returned the questionnaires (24 of 34 for the treatment group and 20 out of 30 for the control group). Most of the families from whom we did not receive questionnaires had moved and we were unable to locate their new address. This study is preliminary and exploratory.
One hundred percent of the control group families had sought and continued in treatment with other treatment providers, with an average of 50 sessions. None of these families received DDP. As will be shown, despite receiving extensive treatment, the control group actually exhibited an increase in symptoms over the 3.3 years. Forty-two percent of the treatment group received treatment after completing DDP. Most of this continued treatment was for co-morbid conditions, such as Bipolar Disorder and Attention Deficit/Hyperactivity Disorder. The majority of the children in the treatment group who received continued treatment after competing DDP received medication management treatment.
Participants
Details about sample selection can be found in Becker-Weidman (2006). The average age at adoption was 7 years and the average number of episodes of prior treatment was 3.4 (82% of the children in the treatment group and 83% of children in the control group had previously received treatment, but without improvement in symptoms). Families were referred to the Center for Family Development from a variety of sources including departments of social services, physician offices, other mental health providers and clinics, and ‘word of mouth’. All cases selected were from the closed cases files during a one-year period and all children had a primary diagnosis of RAD using the criteria in the DSM IV.
Measures
The Child Behavior Checklist (CBCL) (Achenbach, 1991) is composed of several questionnaires and is a parent-report measure designed to assess behavior problems of children 2 to 18 years of age. The instrument has widely accepted reliability and validity that is reported on extensively in the manual.
The Randolph Attachment Disorder Questionnaire (Randolph, 2000) assesses Attachment Disorder. It consists of 30 items completed by the caregiver who rates each item on a 1–5 scale. The manual (Randolph, 2000) describes in detail the development of the test, scoring, reliability, and validity.
Independent Variable: Dyadic Developmental Psychotherapy
Dyadic Developmental Psychotherapy (Hughes, 1997, 2004, 2005) basic principles are summarized as follows:
1. A focus on both the caregivers’ and therapists’ own attachment strategies. Previous research (Dozier et al., 2001; Tyrell et al., 1999) has shown the importance of the caregiver’s and therapist’s state of mind for the success of interventions.
2. Therapist and caregiver are attuned to the child’s subjective experience and reflect this back to the child. In the process of maintaining an intersubjective attuned connection with the child, the therapist and caregiver help the child regulate affect and construct a coherent autobiographical narrative.
3. Sharing of subjective experiences.
4. Use of PACE and PLACE are essential to healing. PACE refers to the therapist setting a healing pace to therapy by being playful, accepting, curious, and empathic. The idea is that the therapist maintains an emotional connection with the client (attunement) and dyadically regulates the child’s affect. In this manner, the therapist ensures that there is an emotionally meaningful component to treatment without the client becoming dysregulated. PLACE refers to the parent creating a healing environment by being playful, loving, accepting, curious, and empathic. These ideas are described more fully below.
1. Directly address the inevitable misattunements and conflicts that arise in interpersonal relationships.
2. Caregivers use attachment-facilitating interventions.
3. Use of a variety of interventions, including cognitive-behavioral strategies.
Dyadic Developmental Psychotherapy interventions flow from several theoretical and empirical lines (Becker-Weidman and Shell, 2005). Attachment theory (Bowlby, 1980, 1988) provides the theoretical foundation for DDP. Early trauma disrupts the normally developing attachment system by creating distorted internal working models of self, others, and caregivers.
Current thinking and research on the neurobiology of interpersonal behavior (Siegel, 1999, 2001, 2002; Schore, 2001) is another part of the foundation on which DDP rests. The work of Bruce Perry (Perry, 1994) and the Child Trauma Academy describes how trauma affects the developing child in a profound manner and requires special treatment approaches. The works of Siegel, Shore, and others provide a foundation for understanding how early attachment experiences affect brain development and later behavior. The focus of this work on the nature and quality of the attachment relationship support a major focus of DDP of maintaining a positive affectively attuned relationship as central to healing trauma.
The primary approach is to create a secure base in treatment (using techniques that fit with maintaining a healing PACE (Playful, Accepting, Curious, and Empathic) and at home using principles that provide safe structure and a healing PLACE (Playful, Loving, Acceptance, Curious, and Empathic). Developing and sustaining an attuned relationship within which contingent collaborative communication occurs helps the child heal. Healing is facilitated by the co-regulation of affect and the development of greater reflective capacities (Fonagy et al., 2002).
Dyadic Developmental Psychotherapy, as conducted at the Center for Family Development, uses 2-hour sessions involving one therapist, parent(s), and child. Two offices are used. Unless the caregivers are in the treatment room, the caregivers view treatment from another room by closed circuit television or a one-way mirror. The usual structure of a session involves three components. First, the therapist meets with the caregiver in one office while the child is seated in the treatment room. During this part of treatment, the caregiver is instructed in attachment parenting methods (Becker-Weidman and Shell, 2005). The caregiver’s own issues that may create difficulties with developing affective attunement with their child may also be explored and resolved. Effective parenting methods for children with trauma-attachment disorders require a high degree of structure and consistency, along with an affective milieu that demonstrates playfulness, love, acceptance, curiosity, and empathy (PLACE). During this part of the treatment, caregivers receive support and are given the same level of attuned responsiveness that we wish the child to experience. Quite often caregivers feel blamed, devalued, incompetent, depleted, and angry. Parent-support is an important dimension of treatment to help caregivers be more able to maintain an attuned connecting relationship with their child. Second, the therapist, frequently with the caregiver present as well, meets with the child in the treatment room. This generally takes 60–90 minutes. Third, the therapist meets with the caregiver without the child. Broadly speaking, the treatment with the child uses three categories of interventions: affective attunement, cognitive restructuring, and psychodramatic reenactments. Treatment with the caregivers uses two categories of interventions: first, teaching effective parenting methods and helping the caregivers avoid power struggles and, second, maintaining the proper PLACE or attitude. The caregivers provide a high degree of structure to provide safety for the child. Within this structured world, the caregiver maintains a high degree of affective attunement that is nurturing and that repeatedly enacts the attachment-cycle of engagement, disruption, and interactive repair (Siegel, 2001; Schore, 2001).
The treatment provided in this study (DDP) often adhered to a structure with several dimensions (see Figure 1). First, behavior is identified and explored. The behavior may have occurred in the immediate interaction or have occurred at some time in the past. Second, using curiosity and acceptance the behavior is explored and the meaning to the child begins to emerge. Third, empathy is used to reduce the child’s sense of shame and increase the child’s sense of being accepted and understood. Fourth, the child’s behavior is then normalized. In other words, once the meaning of the behavior and its basis in past trauma is identified, it becomes understandable that the symptom is present. An example of such an interaction is the following:
Therapist: ‘Wow, I see how you got so angry when your Mom asked you to pick up your toys. You thought she was being mean and didn’t want you to have fun or love you. You thought she was going to take everything away and leave you like your first Mom did, like when your first Mom took your toys and then left you alone in the apartment that time. Oh, I can really understand now how hard that must be for you when Mom said to clean up. You really felt mad and scared. That must be so hard for you.’
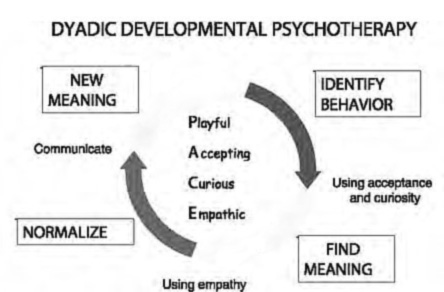
Figure 1. Process Model of Dyadic Development Psychotherapy Fifth, the child communicates this understanding to the caregiver. Sixth, finally, a new meaning for the behavior is found and the child’s actions are integrated into a coherent autobiographical narrative by communicating the new experience and meaning to the caregiver.
Past traumas are revisited by reading documents such as police reports, protective service investigative reports, court documents, and adoption summaries and through psychodramatic reenactments. These interventions, which occur within a safe attuned relationship, allow the child to integrate the past traumas and to understand the past and present experiences that create the feelings and thoughts associated with the child’s behavioral disturbances. The child develops secondary representations of these events, feelings, and thoughts that result in greater affect regulation and a more integrated autobiographical narrative.
Results
The results for the treatment group show that all the scores remain in the normal range and that after nearly 4 years the improvements in the behaviors measured remain clinically and statistically significant. Table 2 shows the scores on the Child Behavior Checklist (CBCL) and Randolph Attachment Disorder Questionnaire (RADQ) for the children in the treatment group. The pre-test measure was taken during the evaluation period before treatment began. The first post-test measure was taken an average of 1.1 years after treatment ended. The treatment group received an average of 23 sessions of DDP over 11 months.
The second post-test measure was taken an average of 4 years after treatment ended. As Table 1 indicates, approximately 50% of the treatment group received additional treatment after DDP ended, but this was primarily medication management treatment.
The control group did not fare as well. As demonstrated in Table 3, all the scores remained in the clinical range despite having received on-going treatment averaging 50 sessions. In addition, there were small but significant increases in Anxious/Depressed symptoms, Attention Problems, Rule-Breaking Behavior, and Aggressive Behavior on the Child Behavior Checklist.
The control group results are of particular concern since all the children received treatment, from various agencies and professionals in private practice, none of whom are affiliated with the Center for Family Development. As the previous study demonstrated, there was no clinically or statistically significant difference between the control and treatment groups on the variables measured before treatment began. There were statistically and clinically significant changes in the behaviors measured for the treatment group, but not for the control group, after the initial one-year follow-up period. These results suggest that DDP is an effective treatment and that the results of this treatment are stable over time.
Past traumas are revisited by reading documents such as police reports, protective service investigative reports, court documents, and adoption summaries and through psychodramatic reenactments. These interventions, which occur within a safe attuned relationship, allow the child to integrate the past traumas and to understand the past and present experiences that create the feelings and thoughts associated with the child’s behavioral disturbances. The child develops secondary representations of these events, feelings, and thoughts that result in greater affect regulation and a more integrated autobiographical narrative.
Results
The results for the treatment group show that all the scores remain in the normal range and that after nearly 4 years the improvements in the behaviors measured remain clinically and statistically significant. Table 2 shows the scores on the Child Behavior Checklist (CBCL) and Randolph Attachment Disorder Questionnaire (RADQ) for the children in the treatment group. The pre-test measure was taken during the evaluation period before treatment began. The first post-test measure was taken an average of 1.1 years after treatment ended. The treatment group received an average of 23 sessions of DDP over 11 months.
The second post-test measure was taken an average of 4 years after treatment ended. As Table 1 indicates, approximately 50% of the treatment group received additional treatment after DDP ended, but this was primarily medication management treatment.
The control group did not fare as well. As demonstrated in Table 3, all the scores remained in the clinical range despite having received on-going treatment averaging 50 sessions. In addition, there were small but significant increases in Anxious/Depressed symptoms, Attention Problems, Rule-Breaking Behavior, and Aggressive Behavior on the Child Behavior Checklist.
The control group results are of particular concern since all the children received treatment, from various agencies and professionals in private practice, none of whom are affiliated with the Center for Family Development. As the previous study demonstrated, there was no clinically or statistically significant difference between the control and treatment groups on the variables measured before treatment began. There were statistically and clinically significant changes in the behaviors measured for the treatment group, but not for the control group, after the initial one-year follow-up period. These results suggest that DDP is an effective treatment and that the results of this treatment are stable over time.
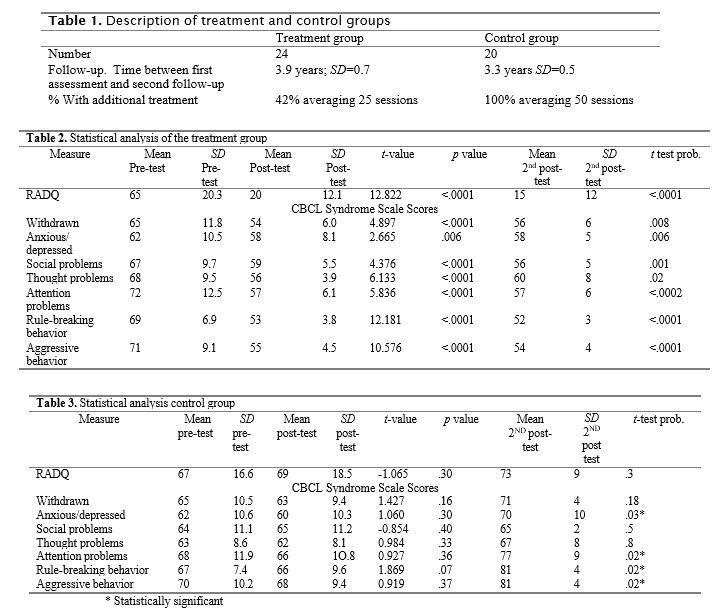
Figure 1. Process Model of Dyadic Development Psychotherapy Fifth, the child communicates this understanding to the caregiver. Sixth, finally, a new meaning for the behavior is found and the child’s actions are integrated into a coherent autobiographical narrative by communicating the new experience and meaning to the caregiver.
Past traumas are revisited by reading documents such as police reports, protective service investigative reports, court documents, and adoption summaries and through psychodramatic reenactments. These interventions, which occur within a safe attuned relationship, allow the child to integrate the past traumas and to understand the past and present experiences that create the feelings and thoughts associated with the child’s behavioral disturbances. The child develops secondary representations of these events, feelings, and thoughts that result in greater affect regulation and a more integrated autobiographical narrative.
Results
The results for the treatment group show that all the scores remain in the normal range and that after nearly 4 years the improvements in the behaviors measured remain clinically and statistically significant. Table 2 shows the scores on the Child Behavior Checklist (CBCL) and Randolph Attachment Disorder Questionnaire (RADQ) for the children in the treatment group. The pre-test measure was taken during the evaluation period before treatment began. The first post-test measure was taken an average of 1.1 years after treatment ended. The treatment group received an average of 23 sessions of DDP over 11 months.
The second post-test measure was taken an average of 4 years after treatment ended. As Table 1 indicates, approximately 50% of the treatment group received additional treatment after DDP ended, but this was primarily medication management treatment.
The control group did not fare as well. As demonstrated in Table 3, all the scores remained in the clinical range despite having received on-going treatment averaging 50 sessions. In addition, there were small but significant increases in Anxious/Depressed symptoms, Attention Problems, Rule-Breaking Behavior, and Aggressive Behavior on the Child Behavior Checklist.
The control group results are of particular concern since all the children received treatment, from various agencies and professionals in private practice, none of whom are affiliated with the Center for Family Development. As the previous study demonstrated, there was no clinically or statistically significant difference between the control and treatment groups on the variables measured before treatment began. There were statistically and clinically significant changes in the behaviors measured for the treatment group, but not for the control group, after the initial one-year follow-up period. These results suggest that DDP is an effective treatment and that the results of this treatment are stable over time.
Discussion and Conclusions
The purpose of the present study was to demonstrate the longer term effectiveness of Dyadic Developmental Psychotherapy with children who have trauma-attachment disorders. Children with the symptoms of attachment disorder and antisocial behaviors are very likely to continue these behaviors in adulthood (Robins and Price, 1991; Loeber, 1991). In addition, children with trauma-attachment disorders are more likely to develop severe personality disorders, such as Borderline Personality Disorder, Sociopathic Personality Disorder, Narcissistic Personality Disorder, and other personality disorders in adulthood (Dozier et al., 1999). For these reasons, it is vital that effective treatment for children with trauma-attachment problems be developed and validated. DDP appears to be one such treatment.
This study found statistically and clinically significant reductions in outcome variables that continued 4 years after treatment ended. The basis for these changes is that an affectively based treatment will result in integration of trauma, improved affect regulation, and an enhanced, integrated, and coherent autobiographical sense of self. It is suggested that treatment allows the child to develop a healthier attachment to the child’s caregiver, increase the child’s capacity for self-regulation, empathy, remorse, and toleration of higher levels of stress. The measurable dimensions of these changes are seen in a number of areas:
1. Increased capacity to use the caregiver as a secure base for comfort and security as measured by a decrease in Withdrawn/Depressed symptoms;
2. Reduction in grief and loss issues associated with abuse, neglect, and foster/adoptive placements as measured by a reduction in the Depressed/Anxious problems;
3. Improved ability to form social relationships as measured by a reduction in Social Problems. While a reduction in social problems does not guarantee improved ability to form social relationships, the reduction in these problems removes a significant barrier to the formation of healthy and developmentally appropriate social relationships;
4. Improved cause-effect thinking as measured by a decrease in Thought Problems;
5. Reduced aggression;
6. Increased adherence to generally acceptable social behavior as measured by a reduction in Delinquent Behavior.
The conclusion that DDP may be the cause of the clinically and statistically significant reductions in the measured outcome variables is bolstered by the use of a control group. The control group was not statistically different from the treatment-group on such variables as age, gender, race, type of adoption, age at adoption, or number of prior treatment episodes. Furthermore, while the treatment groups continued to exhibit behavior within the normal range, the control group’s behavior actually worsened; this was despite the fact that the control group received an average of 50 treatment sessions (not DDP) in the intervening period.
The treatment group received DDP while 53% of the original control group received ‘usual-care’ but not DDP; the other 43% did not receive treatment of any kind. However, 100% of this control group received treatment during the second follow-up period, while their behavior worsened. This finding strengthens the conclusion that DDP is an effective method of treating children with attachment-trauma disorders. Individual therapy, play therapy, family therapy, residential treatment, and intensive outpatient treatment are the usual treatment modalities that these children receive. The lack of change and actual worsening in the control group’s measured outcome variables bolsters the con- clusion that ‘usual care’ methods are not effective in treating such abused and maltreated children while DDP is an effective treatment method.
It is hypothesized that Dyadic Developmental Psychotherapy is effective because of its reliance on and development of affective attunement between therapist and child, caregiver and child, and therapist and caregiver. This would be a fruitful area for further research. Using a process measure of affective attunement before, during and after treatment would be one way to explore whether affective attunement may be an active ingredient in DDP. Furthermore, DDP’s significant involvement of caregivers in treatment facilitates the development of an affectively attuned relationship between the child and caregiver. Within the safety of the attuned relationship the shame of past trauma and current misbehaviors are explored, experienced, and integrated. The caregiver-child interactions build on a dyadic affect regulation process that normally occurs during infancy and the toddler years. DDP facilitates the development of a healthy attachment between child and caregiver, enables the child to affectively trust the caregiver, and allows the child to secure comfort and safety from the caregiver.
A limitation of this study is that there was no direct reliable and valid measure of attachment between child and caregiver. There are no existing reliable and valid measures of child-caregiver attachment for the age group in this study; developing such a measure that can be used in a clinic or office setting should be a priority. Anecdotally, we can report a nearly universal improvement in the treatment group in reported secure base behaviors. For example, before treatment most of the children did not go to their caregiver for care, comfort, or solace. After treatment, there was a marked increase in reports of such use of the caregiver for comfort in times of stress or discomfort. We also found that the treatment group caregivers reported a more authentic and genuine affective relationship with their child. The children were experienced as more spontaneous in their displays of affection (without using affection in a manipulative manner). Children also reported more enjoyment of their caregivers and more interest in seeking out their advice, ideas, approval, and assistance. However, anecdotal evidence of an increase in attachment behaviors lacks the power of a more rigorous and empirically based measure.
Another limitation is that the measures used were all caregiver report and subject to respondent bias. However, since the treatment group and control group were not statistically different on any of the pre-test measure and on a variety of demographic variables, this seems to be a more remote possible limitation. Other limitations and confounding issues include the fact that in this study the two components of the DDP treatment process (work with caregiver and direct work with the child) were not separately evaluated. An area for future research would be to look at these two components to determine whether both are necessary and to what extent each contributes to a successful outcome. For example, since the attachment classification of the caregiver has such a profound impact on the child’s pattern and style of attachment, what is the impact of work with the caregiver and would working only with the caregiver produce significant changes in the child or is the direct work with the child also a necessary component? We suspect that, given the current thinking on the treatment of Complex Trauma among children and adolescents (Briere and Scott, 2006; Cook et al., 2005), that direct work with the child is essential for a favorable outcome, but this remains to be empirically tested.
Dyadic Developmental Psychotherapy is a family therapy based on Attachment Theory (Bowlby 1980, 1988; Holmes, 1993). It is an amalgamation of several approaches, methods and techniques that have a strong evidence base. DDP uses a variety of interventions and methods with a well established foundation. For example, this treatment method’s approach is consistent with the basic principles of effective treatment for complex trauma (Cook et al., 2003, 2005). These authors identify six core components of complex trauma interventions: ‘safety, self-regulation, self- reflective information processing, traumatic experience integration, relational engagement, and positive affect enhancement’ (Cook et al, 2005 p. 395). DDP emphasizes each of these six core components.
Specific components, methods and principles of DDP that have good empirical support and are shared with other treatment approaches (Orlinsky, Grawe, and Parks, 1994) include the following:
1. Affect arousal, a focus on problems of living and on core personal relationships are elements of DDP that have been shown to be important for positive outcomes for treatment.
2. Explaining how the past may continue to effect present behavior and emotions, interpretation, has been found to be an effective mode of intervention.
3. Forming and maintaining a therapeutic bond is a core component of DDP. The use of PACE is designed specifically to help facilitate this. There is a significant positive association between outcome and the therapeutic bond (66% of the studies with an effect size of at least .25 in one quarter of the studies, p.308). In looking at the therapist’s contribution to the therapeutic bond, a significant positive association with outcome was found: ‘The therapist’s contribution was positively associated with outcome 67% of the time and never negatively implicated.’ (p. 321). ‘The strongest evidence linking process to outcome concerns the therapeutic bond or alliance.’ (p. 360).
4. Acceptance is a significant dimension of the practice of DDP. Therapist affirmation (acceptance, non-possessive warmth, or positive regard) was found to be a significant factor in positive therapeutic outcome.
Overall such factors as empathy, the capacity for reflection, intersubjective sharing of affect, the therapeutic alliance, furthering reflection, deepening emotional processing, enhancing adaptive skills, developing and maintaining the therapeutic bond, therapist affirmation, communication attunement, and the bond of relatedness between therapist and patient are all important factors in psychotherapy outcome and are all important elements of DDP.
This study supports several of O’Connor and Zeanah’s (2003) conclusions and recommendations concerning treatment. They contended that ‘treatments for children with attachment disorders should be promoted only when they are evidence-based’ (p. 241). The results of this study are a beginning toward that end. While there are a number of limitations to this study, given the severity of the disorders in question, the paucity of effective treatments, and the desperation of caregivers seeking help, it is a step in the right direction. DDP is not a coercive therapy, which can be dangerous. DDP provides caregiver support as an integral part of its treatment methodologies. Finally, DDP uses a multimodal approach built around affect attunement. This study therefore indicates that DDP is an effective intervention for children with trauma-attachment problems. Additional research with a larger sample would be a valuable extension of this study.
Outcome Research Controls
Research References
Article - Trends in Research by Arthur Becker-Weidman, Ph.D.
Past traumas are revisited by reading documents such as police reports, protective service investigative reports, court documents, and adoption summaries and through psychodramatic reenactments. These interventions, which occur within a safe attuned relationship, allow the child to integrate the past traumas and to understand the past and present experiences that create the feelings and thoughts associated with the child’s behavioral disturbances. The child develops secondary representations of these events, feelings, and thoughts that result in greater affect regulation and a more integrated autobiographical narrative.
Results
The results for the treatment group show that all the scores remain in the normal range and that after nearly 4 years the improvements in the behaviors measured remain clinically and statistically significant. Table 2 shows the scores on the Child Behavior Checklist (CBCL) and Randolph Attachment Disorder Questionnaire (RADQ) for the children in the treatment group. The pre-test measure was taken during the evaluation period before treatment began. The first post-test measure was taken an average of 1.1 years after treatment ended. The treatment group received an average of 23 sessions of DDP over 11 months.
The second post-test measure was taken an average of 4 years after treatment ended. As Table 1 indicates, approximately 50% of the treatment group received additional treatment after DDP ended, but this was primarily medication management treatment.
The control group did not fare as well. As demonstrated in Table 3, all the scores remained in the clinical range despite having received on-going treatment averaging 50 sessions. In addition, there were small but significant increases in Anxious/Depressed symptoms, Attention Problems, Rule-Breaking Behavior, and Aggressive Behavior on the Child Behavior Checklist.
The control group results are of particular concern since all the children received treatment, from various agencies and professionals in private practice, none of whom are affiliated with the Center for Family Development. As the previous study demonstrated, there was no clinically or statistically significant difference between the control and treatment groups on the variables measured before treatment began. There were statistically and clinically significant changes in the behaviors measured for the treatment group, but not for the control group, after the initial one-year follow-up period. These results suggest that DDP is an effective treatment and that the results of this treatment are stable over time.
Discussion and Conclusions
The purpose of the present study was to demonstrate the longer term effectiveness of Dyadic Developmental Psychotherapy with children who have trauma-attachment disorders. Children with the symptoms of attachment disorder and antisocial behaviors are very likely to continue these behaviors in adulthood (Robins and Price, 1991; Loeber, 1991). In addition, children with trauma-attachment disorders are more likely to develop severe personality disorders, such as Borderline Personality Disorder, Sociopathic Personality Disorder, Narcissistic Personality Disorder, and other personality disorders in adulthood (Dozier et al., 1999). For these reasons, it is vital that effective treatment for children with trauma-attachment problems be developed and validated. DDP appears to be one such treatment.
This study found statistically and clinically significant reductions in outcome variables that continued 4 years after treatment ended. The basis for these changes is that an affectively based treatment will result in integration of trauma, improved affect regulation, and an enhanced, integrated, and coherent autobiographical sense of self. It is suggested that treatment allows the child to develop a healthier attachment to the child’s caregiver, increase the child’s capacity for self-regulation, empathy, remorse, and toleration of higher levels of stress. The measurable dimensions of these changes are seen in a number of areas:
1. Increased capacity to use the caregiver as a secure base for comfort and security as measured by a decrease in Withdrawn/Depressed symptoms;
2. Reduction in grief and loss issues associated with abuse, neglect, and foster/adoptive placements as measured by a reduction in the Depressed/Anxious problems;
3. Improved ability to form social relationships as measured by a reduction in Social Problems. While a reduction in social problems does not guarantee improved ability to form social relationships, the reduction in these problems removes a significant barrier to the formation of healthy and developmentally appropriate social relationships;
4. Improved cause-effect thinking as measured by a decrease in Thought Problems;
5. Reduced aggression;
6. Increased adherence to generally acceptable social behavior as measured by a reduction in Delinquent Behavior.
The conclusion that DDP may be the cause of the clinically and statistically significant reductions in the measured outcome variables is bolstered by the use of a control group. The control group was not statistically different from the treatment-group on such variables as age, gender, race, type of adoption, age at adoption, or number of prior treatment episodes. Furthermore, while the treatment groups continued to exhibit behavior within the normal range, the control group’s behavior actually worsened; this was despite the fact that the control group received an average of 50 treatment sessions (not DDP) in the intervening period.
The treatment group received DDP while 53% of the original control group received ‘usual-care’ but not DDP; the other 43% did not receive treatment of any kind. However, 100% of this control group received treatment during the second follow-up period, while their behavior worsened. This finding strengthens the conclusion that DDP is an effective method of treating children with attachment-trauma disorders. Individual therapy, play therapy, family therapy, residential treatment, and intensive outpatient treatment are the usual treatment modalities that these children receive. The lack of change and actual worsening in the control group’s measured outcome variables bolsters the con- clusion that ‘usual care’ methods are not effective in treating such abused and maltreated children while DDP is an effective treatment method.
It is hypothesized that Dyadic Developmental Psychotherapy is effective because of its reliance on and development of affective attunement between therapist and child, caregiver and child, and therapist and caregiver. This would be a fruitful area for further research. Using a process measure of affective attunement before, during and after treatment would be one way to explore whether affective attunement may be an active ingredient in DDP. Furthermore, DDP’s significant involvement of caregivers in treatment facilitates the development of an affectively attuned relationship between the child and caregiver. Within the safety of the attuned relationship the shame of past trauma and current misbehaviors are explored, experienced, and integrated. The caregiver-child interactions build on a dyadic affect regulation process that normally occurs during infancy and the toddler years. DDP facilitates the development of a healthy attachment between child and caregiver, enables the child to affectively trust the caregiver, and allows the child to secure comfort and safety from the caregiver.
A limitation of this study is that there was no direct reliable and valid measure of attachment between child and caregiver. There are no existing reliable and valid measures of child-caregiver attachment for the age group in this study; developing such a measure that can be used in a clinic or office setting should be a priority. Anecdotally, we can report a nearly universal improvement in the treatment group in reported secure base behaviors. For example, before treatment most of the children did not go to their caregiver for care, comfort, or solace. After treatment, there was a marked increase in reports of such use of the caregiver for comfort in times of stress or discomfort. We also found that the treatment group caregivers reported a more authentic and genuine affective relationship with their child. The children were experienced as more spontaneous in their displays of affection (without using affection in a manipulative manner). Children also reported more enjoyment of their caregivers and more interest in seeking out their advice, ideas, approval, and assistance. However, anecdotal evidence of an increase in attachment behaviors lacks the power of a more rigorous and empirically based measure.
Another limitation is that the measures used were all caregiver report and subject to respondent bias. However, since the treatment group and control group were not statistically different on any of the pre-test measure and on a variety of demographic variables, this seems to be a more remote possible limitation. Other limitations and confounding issues include the fact that in this study the two components of the DDP treatment process (work with caregiver and direct work with the child) were not separately evaluated. An area for future research would be to look at these two components to determine whether both are necessary and to what extent each contributes to a successful outcome. For example, since the attachment classification of the caregiver has such a profound impact on the child’s pattern and style of attachment, what is the impact of work with the caregiver and would working only with the caregiver produce significant changes in the child or is the direct work with the child also a necessary component? We suspect that, given the current thinking on the treatment of Complex Trauma among children and adolescents (Briere and Scott, 2006; Cook et al., 2005), that direct work with the child is essential for a favorable outcome, but this remains to be empirically tested.
Dyadic Developmental Psychotherapy is a family therapy based on Attachment Theory (Bowlby 1980, 1988; Holmes, 1993). It is an amalgamation of several approaches, methods and techniques that have a strong evidence base. DDP uses a variety of interventions and methods with a well established foundation. For example, this treatment method’s approach is consistent with the basic principles of effective treatment for complex trauma (Cook et al., 2003, 2005). These authors identify six core components of complex trauma interventions: ‘safety, self-regulation, self- reflective information processing, traumatic experience integration, relational engagement, and positive affect enhancement’ (Cook et al, 2005 p. 395). DDP emphasizes each of these six core components.
Specific components, methods and principles of DDP that have good empirical support and are shared with other treatment approaches (Orlinsky, Grawe, and Parks, 1994) include the following:
1. Affect arousal, a focus on problems of living and on core personal relationships are elements of DDP that have been shown to be important for positive outcomes for treatment.
2. Explaining how the past may continue to effect present behavior and emotions, interpretation, has been found to be an effective mode of intervention.
3. Forming and maintaining a therapeutic bond is a core component of DDP. The use of PACE is designed specifically to help facilitate this. There is a significant positive association between outcome and the therapeutic bond (66% of the studies with an effect size of at least .25 in one quarter of the studies, p.308). In looking at the therapist’s contribution to the therapeutic bond, a significant positive association with outcome was found: ‘The therapist’s contribution was positively associated with outcome 67% of the time and never negatively implicated.’ (p. 321). ‘The strongest evidence linking process to outcome concerns the therapeutic bond or alliance.’ (p. 360).
4. Acceptance is a significant dimension of the practice of DDP. Therapist affirmation (acceptance, non-possessive warmth, or positive regard) was found to be a significant factor in positive therapeutic outcome.
Overall such factors as empathy, the capacity for reflection, intersubjective sharing of affect, the therapeutic alliance, furthering reflection, deepening emotional processing, enhancing adaptive skills, developing and maintaining the therapeutic bond, therapist affirmation, communication attunement, and the bond of relatedness between therapist and patient are all important factors in psychotherapy outcome and are all important elements of DDP.
This study supports several of O’Connor and Zeanah’s (2003) conclusions and recommendations concerning treatment. They contended that ‘treatments for children with attachment disorders should be promoted only when they are evidence-based’ (p. 241). The results of this study are a beginning toward that end. While there are a number of limitations to this study, given the severity of the disorders in question, the paucity of effective treatments, and the desperation of caregivers seeking help, it is a step in the right direction. DDP is not a coercive therapy, which can be dangerous. DDP provides caregiver support as an integral part of its treatment methodologies. Finally, DDP uses a multimodal approach built around affect attunement. This study therefore indicates that DDP is an effective intervention for children with trauma-attachment problems. Additional research with a larger sample would be a valuable extension of this study.
Outcome Research Controls
Research References
Article - Trends in Research by Arthur Becker-Weidman, Ph.D.